Neck Care, Cochrane Systematic Reviews and Knowledge Translation: Anita Gross
Submitted by: Anita Gross, PT, MSc
A frequent criticism of Cochrane reviews and other systematic reviews is that, in spite of their methodological rigor, they fail to provide clear clinical answers or lack appropriate translation of the evidence into the realities of clinical practice. It is common to read in reviews that “the methodological quality of the evidence is limited, there are too few studies of merit, or there are no clear evidence-based answers.” This criticism is also valid of the “conservative management of mechanical neck disorders” systematic reviews delivered by the Cervical Overview Group (COG). Others have struggled with this issue, as exemplified in a recent best-evidence synthesis by the Bone and Joint Decade (Hurwitz et al. 2008). While best-evidence synthesis has some methodological differences from the Cochrane reviews, such as design criteria for selection of studies and criteria for methodological quality, its numerous findings overlap substantially with those of the COG. However, these publications have not been prepared in a manner that allows ready uptake by clinicians. Disappointingly, over the past decade, there has been limited improvement in the methodological quality of controlled trials conducted in manual therapy and exercise for neck disorders (Figure 1), in spite of the strong recommendations on conduct and reporting of clinical trials from the Consolidated Standards of Reporting Trials (CONSORT) group and its resulting guidelines (Boutron 2008). Practitioners, however, often have to make practice decisions in the absence of research data of optimal quality. Our team is mindful to highlight the best available evidence, even though it may not be based on optimal methodological rigor, in an attempt to rationally guide clinical practice. WCPT has noted that “Physical therapists have been slow adopters of new technologies – and must learn to overcome common barriers and concerns if their patients are ultimately to benefit” (WCPT 2011). The reasons why social networking (such as Facebook and Twitter), blogs, e-learning, and “wikis” have not been embraced more wholeheartedly by physical therapists and their managers, given the potential benefits for spreading expertise and patient education is not fully understood. Some (WCPT 2011) raised important issues such as: concerns over privacy and patient confidentiality; the lack of academic rigor in much internet information; professional resistance to change; the dull experience of many e-learning packages; institutional/employer resistance to professionals spending time on social networks. COG supports the importance of new technologies for providing healthcare information to low and middle income countries. The publication of research and open access journals over the internet help to impact professional development. COG has taken the following two steps in this regards in the past decade:
Step 1. We have linked our Cochrane Reviews with the development of two simple clinical guides that are complementary – a Clinician Tool Kit (Miller et al 2012) and a Patient Decision Aide (Miller, Gross, MacDermid 2012). They can be found on a
Physical therapy “wiki site” (www.physio-pedia.com – Physiopaedia). Publishing in this open access location allows maximum access to a broad audience. The purpose of ‘Manual therapy and exercise for neck pain: clinical treatment tool-kit’ is to provide a resource for clinical decision making by providing evidence, techniques, and dosages for the use of manual therapy and exercise in the treatment of neck pain.
We have included the actual magnitude of effects in this tool. The magnitude of expected benefit can be important to patients, third-party payers, and policymakers. It can be represented in clinical trials as the absolute benefit as well as the number-needed-to-treat (NNT)*. The evidence included in this knowledge translation tool suggests between 2 to 5 patients with subacute or chronic mechanical neck disorders (with or without headache) would need to be treated for 1 patient to substantially benefit (Miller et ql 2010). NNTs in the range of 2 to 5 are generally considered to indicate important treatment effects. The clinical tool-kit in this wiki site serve as the most straightforward clinical treatment guide for the disorders encompassed by the term “neck pain.” They depict both the evidence in terms of its direction (evidence for its use, or against its use), as well as data on specific treatment techniques and dosages. Many clinicians have a positive attitude towards evidence-based practice, but may not have the time or resources to seek out the specific technique and dosage information from positive trials investigating the effectiveness of treatment strategies. Knowledge translation tools can be used to help clinicians access the evidence provided in systematic reviews and provide the specific technique and dosage information so that it can be implemented in clinical practice. In spite of thousands of hits a month on this wiki site for this topic, the overarching question of “Does accessing these tool actually influence practice?” eludes us.
Step 2: We have linked with the ICON (International Collaboration on Neck) project (MacDermid, Miller and Gross 2013). This project’s goal was to develop and deliver overviews on neck care through open access journals (Peloso et al 2013; Graham et al 2013; Gross et al 2013). Have you accessed them yet? Both COG and ICON are also currently linking with AAOMPT to update their clinical guidelines (Childs et al 2008). Clinical practice guidelines are defined as “systematically developed statements to assist practitioner and patient decisions about appropriate healthcare for specific circumstances.” (Hasenfeld & Shekelle 2003) Ideally, they serve as a “knowledge translation tool” to move the best evidence into clinical practice. However, some guidelines are not based on high-quality evidence (Hasenfeld & Shekelle 2003), such as that found in systematic reviews. Systematic reviews facilitate clinicians’ ability to stay current, as they compile high-quality, synthesized data. Guidelines commonly exhibit discrepancies and may not be evidence based. The onus is on the clinician to judiciously interpret and integrate the information provided.
In this decade of information explosion, we need to be more engaged. There is a wide spectrum of treatments available to people with neck pain, not all of which are equally effective. We need to be a tech savvy profession, we need to be continuously involved in knowledge engagement, critical analysis, knowledge generation (research involvement), and translate this best evidence into our care, our local/regional policy development and governance decision making. “Are you engaged?”
References
Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann Intern Med. 2008;148:295-309.
Childs JD, Cleland JA, Elliott JM, et al. Neck Pain: Clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physiotherapy association. JOSPT 2008;38(9):A1-A34.
Graham N, Gross AR, Carlesso LC, Santaguida PL, MacDermid JC, Walton DM, Ho E, ICON. An ICON overview on physical modalities for neck pain and associated disorders. The Open Orthopaedics Journal, 2013, 7, Suppl 4: M6: 440-460.
Gross AR, Kaplan F, Huang S, Khan M, Santaguida PL, Carlesso LC, MacDermid JC, Walton DM, Kenardy J, Söderlund A, Verhagen A, Hartvigsen J. Psychological Care, Patient Education, Orthotics, Ergonomics and Prevention for Neck Pain: A Systematic Overview Update as part of the ICON* Project. The Open Orthopaedics Journal, 2013, 7, (Suppl 4: M12): Sep 20;7:530-61.
Hasenfeld R, Shekelle PG. Is the methodological quality of guidelines declining in the US? Comparison of the quality of US Agency for Health Care Policy and Research (AHCPR) guidelines with those published subsequently. Qual Saf Health Care. 2003;12:428-434.
Hurwitz EL, Carragee EJ, van der Velde G et al. Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine.2008;33:S123-152.
MacDermid JC, Miller J, Gross A: Knowledge Translation Tools are Emerging to Move Neck Pain Research into Practice. The Open Orthopaedics Journal, 7, (Suppl 4: M15):582-593. 2013.
Miller J, Gross A, D’Sylva J, Burnie SJ, Goldsmith CH, Graham N, Haines T, Brønfort G, Hoving JL. Manual therapy and exercise for neck pain: a systematic review. Man Ther 2010 Aug;15(4):334-54. doi:10.1016/j.math.2010.02.007
Miller J, Gross A, Rogers T, Willemse J. Manual Therapy and Exercise for Neck Pain: Clinical Treatment Tool-kit Physiopaedia, March 2012. <http://www.physio-pedia.com/Manual_Therapy_and_Exercise_for_Neck_Pain:_Clinical_Treatment_Tool-kit>
Miller J, Gross A, MacDermid J, COG, ICON. Should I receive manual therapy and exercise for my neck pain?: A patient decision aid. February 2012, <http://www.physio-pedia.com/Should_I_receive_manual_therapy_and_exercise_for_my_neck_pain%3F:_A_patient_decision_aid?utm_source=May+2012&utm_campaign=Physiopedia+Newsletter&utm_medium=socialshare>
Peloso PM, Khan M, Gross AR, Carlesso L, Santaguida PL, Lowcock J, MacDermid JC, Walton D, Goldsmith CH, Langevin P, Shi Q. Pharmacological Interventions including Medical Injections for Neck Pain: An Overview as part of the ICON* Project. The Open Orthopaedics Journal, 2013, 7 (Suppl 4: M8): 473-493.
WCPT News July 2011 < http://www.wcpt.org/intranet/news/list/42659/pdf_article/WCPTNews_July%2… access July 2014.
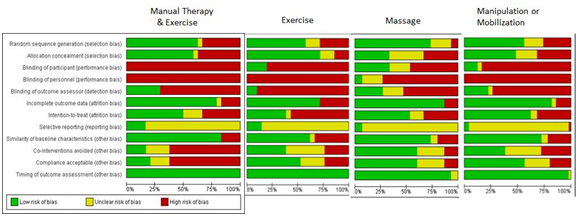
Figure 1. Risk of bias criteria across primary trials in 1) manual therapies as a stand-alone treatment, 2) exercise and 3) manual therapy and exercise primary trials for neck pain.

Connect With PSD!
